Compulsory Vaccination and rates of Coverage Immunisation in Europe
Introduction
High rates of vaccination coverage in childhood are main indicators for public health. However, reaching and maintaining such a target is not always an easy task for public health institutions, and the spread of vaccine refusal and hesitancy is making this even harder.
Enforcing mandatory vaccinations is one of the strategies that some countries adopted and others are considering in order to face this issue. Depending on local legislations, legal consequences for those who do not accept the uptake can be very different, ranging from pecuniary penalties to hurdles to attend public schools. In some cases, parents may even incur penal consequences, as it recently happened in France, were two parents refusing to vaccinate their children risked a jail sentence. Nevertheless, the efficacy of such an approach has been questioned.
ASSET performed an analysis on the issue, comparing coverage rates of immunisation against polio (Pol3), measles (MCV1) and pertussis containing vaccines (DTP3)* in European Union/European Economic Area (EU/EEA) countries, where, according to different policies, these vaccinations are either mandatory or recommended.
This comparison cannot confirm any relationship between mandatory vaccination and rates of childhood immunization in the EU/EEA countries.
* In some countries, such as Italy, vaccination against pertussis is highly recommended but not compulsory, while those against diphteria and tetanus on the contrary are, but the three are usually administered in one single shot.
Methods
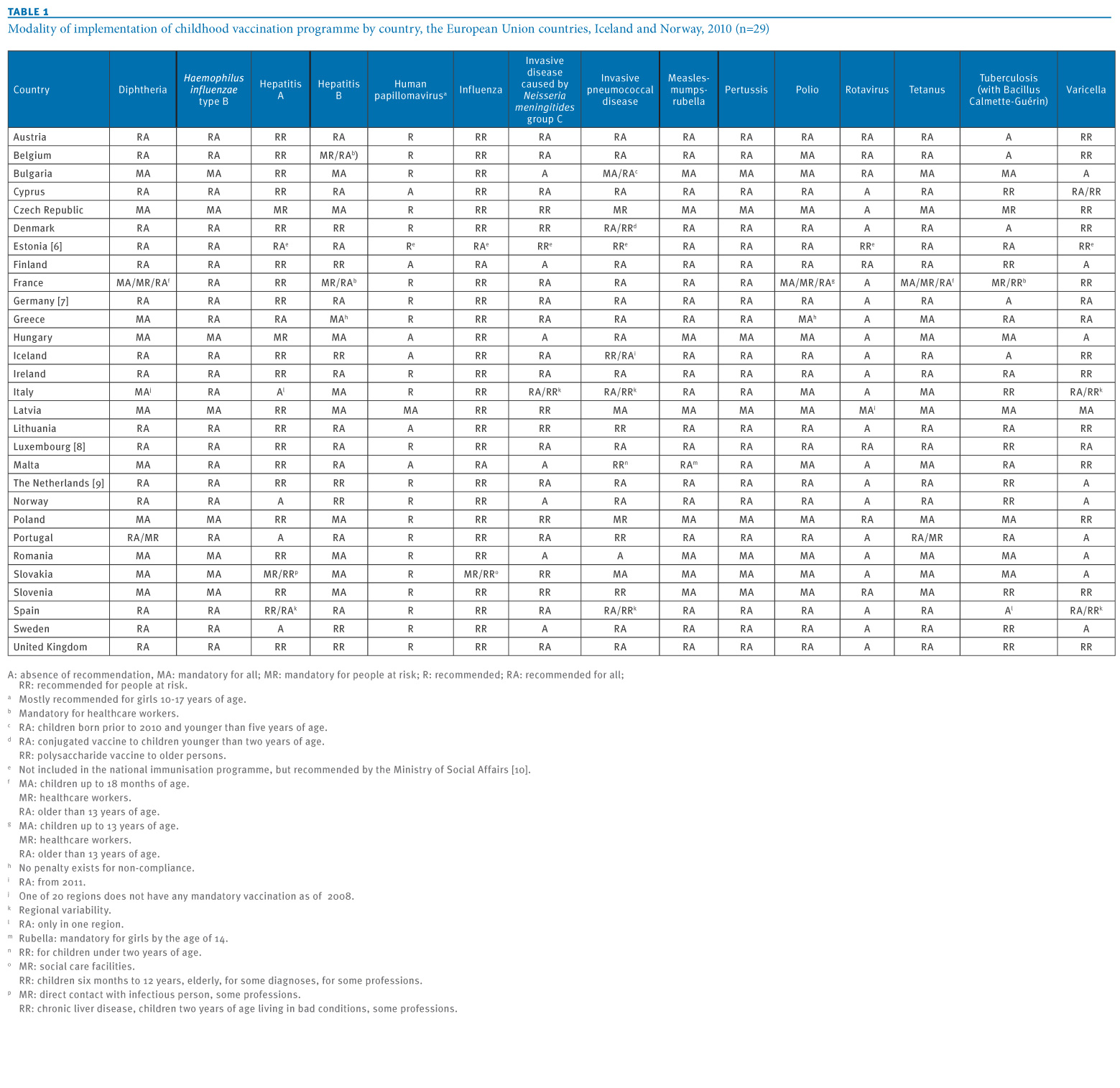
Information on policies of mandatory or recommended vaccinations in the EU/EEA countries were gathered by VENICE project (eurosurveillance.org).
{kind=link}
Data on childhood immunisation coverage in the EU/EEA countries were taken from the UNICEF official website (data.unicef.org). They refer to the period from 2007 to 2013, so that the visualization can show temporal trends in immunisation rate in each country, as well.
As defined by VENICE project, vaccinations are recommended when included in the national immunisation programme for all or some specific groups independent of being funded or not. A vaccine is defined as mandatory if every child must receive it by law without the possibility for the parent to choose to accept the uptake or not, regardless of whether a legal or economical implication exists for the refusal. Law enforcement and legal consequences may be very different but, since the national contexts are difficult to evaluate, the VENICE survey did not collect any information about them.
We chose three relevant vaccinations, on which different policies have been adopted in different countries. While polio vaccine is mandatory in many countries, pertussis vaccine is more often only recommended, even in countries where other vaccinations are compulsory. Measles vaccination is an important indicator of hesitancy and refusal, since misinformation accusing it of causing autism, despite evidence of its fraudulent source, is still going on.
Data Visualization
In the following maps, one for each vaccine, countries where a vaccination is mandatory has been marked with a lined background, while those where the same vaccination is recommended have a spotted background.
Countries coloured in green have had an average higher vaccine coverage than the EU/EEA average – evaluated on all the countries over the period considered – while the coverage is lower than the average in the blue ones.
No evident correlation between colours and different backgrounds appears from the maps.



While maps can give a first, general overview at a glance, the following graphs further analyse the situation by showing the rates of immunization for Pol3, MCV1 and DTP3 vaccines in all EU/EEA countries from 2007 to 2013.
The black line shows the EU/EEA average, evaluated on all the countries, at the time, while green and blue areas indicate coverage, respectively higher or lower than the average, for each country and each vaccine.
The choice of showing the whole 0-100% range in the immunization rates, even if differences are always smaller, highlights countries where the vaccination coverage is significantly different from the average. As with previous maps, graphs consider if a vaccine is either mandatory or recommended: for each country, a spotted background indicates that a vaccine is recommended, while a lined background indicates that it is mandatory.
{kind=link}

Discussion
This data visualization, showing temporal trends in immunisation rates in the EU/EEA countries in the last years for 3 main vaccines, does not suggest any evident relationship between vaccination coverage and national policies on compulsory vaccinations.
Some examples from the graphs confirm this idea. On one side, countries where a vaccination is mandatory do not usually reach better coverage than neighbour or similar countries where there is no legal obligation, as one can see comparing both Baltic and Scandinavian countries.


On the other side, similarly negative trends in very different countries, with different policies about compulsory vaccination, suggest that other factors could be involved, ie. not only hesitancy in parents, but also difficulties of healthcare systems in reaching all children.

Conclusions
This analysis has some limits. One is the lack of information on possible changes in national vaccination policies (recommended or mandatory) over the years, so preventing the possibility to understand if, in any case, a different approach could have influenced trends of immunisation. Thus, gathering these data will be a key step for future analysis.
We analysed data from only three relevant childhood vaccinations, assuming that they can reflect a general situation of immunisation rates in the EU/EEA countries.
Anyway, the analysis could be extended to other vaccinations in the future. Even if this data visualization cannot provide full evidence of the efficacy or inefficacy of mandatory vaccinations on immunisation rates, it shows that this approach does not appear to be relevant in determining childhood immunisation rate in the EU/EEA countries.
Further analysis of maps and graphs could suggest new directions for further investigation.